Process Improvement
Abstract
Background
Tacit clinical knowledge acquired by front-line nurses over many years of practice is notoriously difficult to capture and codify. The knowledge is underpinned by “first-hand” semantics which describe “real world” patient care processes. Possibly, “second-hand” semantics, that is, semantics obtained from nursing focus groups, document review or databases may be used in data sets or electronic health records as “proxy” first-hand semantics. The use of second-hand semantics may have considerable limitations. For example, they may not be a “true” reflection of the original meaning.
Aims
- Enable front-line nurses to capture their own process domain semantics
- Construct ontologies from the semantics and rank semantic similarity.
Method
Underpinning this pilot study is a design science framework in which a purposive sample of four specialist front-line nurses from one Australian hospital each produce one node-to-arc graph depicting a process domain and its semantics. One OWL-DL (Web ontology language-description logic) ontology is constructed from each graph and an automated agent ranks semantic similarity across the four ontologies.esults: Nurses constructed node-to-arc graphs that revealed semantics and processes showing differences in clusters of “responsibility” and different foci on nursing roles. Ontologies were constructed from graphs and the agent found no identical semantics existed across all four ontologies after the terms “patient” and “doctor” were discounted.
Conclusion
From the nurse’s perspective, graphs are a useful “stand-alone” knowledge acquisition tool for the visualization of the process domain and its semantics. Also, the study found that an automated agent can be used to rank semantic similarity across ontologies constructed from graphs.
Introduction
The lack of “first-hand” nursing process semantics
A literature review (Savitz, Jones and Bernard, 2010; Burnes-Bolton, Donaldson, Rutledge, Bennett & Brown, 2007) found little or no evidence of research activity which identifies nursing process semantics, that is, semantics describing what “nurses do.” It is suggested that, in some contexts, the lack of semantics describing the types of services that nurses provide, and their contribution to patient outcomes, has disadvantaged the progress of nursing science and added to so-called nursing “invisibility” in electronic data systems (Butler et al., 2006) .
The challenge of acquiring nursing process semantics, particularly semantics from front-line-nurses, was highlighted by the Institute of Medicine (IOM) (2011). The joint effort produced a comprehensive report to guide the future transformation of the nursing profession. Eight recommendations were tendered. Of most concern to this paper is recommendation eight, which concerns the timely collection and public accessibility of nursing acute health care workforce data. The recommendation identifies the importance of improvements in health data research, particularly focusing on the implementation of efficient data collection and analysis.
The problem this paper addresses
This paper addresses two problems, one flowing from the other. The first problem is the difficulty of obtaining semantics that describe front-line processes from nurses who actually do the work. The second problem is that semantic technology, which is designed to acquire semantics, is difficult to master.
These difficulties may account for the bulk of clinical process studies, designed by computer scientists, resorting to “second-hand” nursing semantics from sources such as documentation (Abidi & Chen, 2006), literature synthesis (Becker, Heine, Herrler, & Krempels, 2003; Din, Abidi, & Jafarpour, 2010; Gooch & Roudsari, 2011; Hurley & Abidi, 2007; Ye, Jiang, Diao, Yang, & Du, 2009) or survey focus groups (Daniyal, Abidi, & Abidi, 2009). As a consequence, semantics not acquired from front-line nurses have been criticised for being used as “proxy” measures that fail to measure the effectiveness of nursing processes.
The use of proxy nursing semantics acquired by non-clinicians has considerable limitations. Gurupur and Tanik (2012) and Anand and Verma (2010) observed that computer scientists are usually not clinicians and clinicians are not computer scientists. This is summed up by Needleman, Kurtzman & Kizer (2007), which explains that process data are difficult to acquire and, consequently, “easier” data often generated from sources previously described are appealing to researchers for their ease of procurement and expedience. It follows that the meaning of second-hand semantics from the proceeding sources may be “lost in translation” and more than likely not be a true reflection of nursing processes. The original idea behind this pilot study was that process semantics may be “unlocked” as front-line nurses construct an ontology which describes their process domain. Semantic technology is one way of acquiring process semantics, but it is not without its limitations.
Semantic technology’s limitations
Semantic technologies, such as ontologies (Appendix B), are designed to acquire semantics describing (in our case) nursing processes. The problem is, ontologies are a machine-readable document, which is a combination of different computer science disciplines, and generally remain a unique domain of computer scientists. Ontology construction is a specialised discipline, so consequently, the construction of ontologies that reflect a nursing reality generally is out of the front-line nurse’s scope.
The solution used in this study
It was determined early in the study that the study’s overhead would be too great in time and resources if front-line nurses constructed ontologies per se. The overhead caused by ontology complexity was addressed by adding an interim step, “node-to-arc graphs” (Appendix A). Nurses use graphs to construct their process domain, and in doing so, capture semantics, entities and relationships that comprise process knowledge. The graphs, in turn, produce the construction language of ontologies.
A database title search in CINAHL, PROQUEST and Google scholar was conducted using the search strings in Table 1. The search period was from 1996 to 2015.
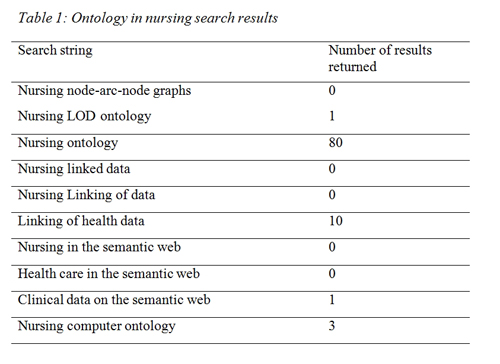
Table 1: Ontology in nursing search results
As seen in Table 1, there were 80 hits returned by the term “nursing ontology” but after review of the abstracts, none were related to the design science methodology used in this pilot study. These journal articles did not discuss computer ontologies, but were concerned with the traditional philosophical definition of ontology as it pertains to the nature of being and reality. The philosophical approach to ontology has dominated nursing literature because nursing science is concerned with different world-views that may help build nursing knowledge. There was no evidence of a nurse constructed computer ontology concerned with describing nursing processes.
The methodology’s underpinnings
This study addresses the lack of nursing process semantics by merging nursing science with semantic technologies. Semantic technologies used in this study are:
- Node-to-arc graphs described in Appendix A
- OWL-DL ontologies described in Appendix B.
The methodology illustrated in Figure 1 underpins the study’s goal to enable front-line nurses to construct their process domains with node-to-arc graphs, ontologies to be constructed from the graphs and the use of an “automated agent” to rank semantics across the ontologies.
To this end, the methodology proceeds in four logical sections. The approach reflects the design science flow from a preliminary stage through to data capture, ontology construction and data evaluation suggested by Peffers et al. (2006).
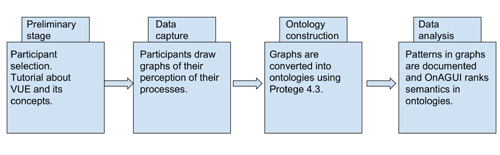
Figure 1: Logical flow in design science framework (Peffers et al., 2006).
Basically, front-line nurses construct their own node-to-arc graphs in simple graphing software, namely, Virtual Understanding Environment (VUE) (Tufts, 2016c) . VUE was chosen because of its uncluttered graphic design and ease of use. VUE has an uncluttered display which front-line nurses can quickly learn and navigate.
The result is a visual graph that reflects the nurse’s perception of a process domain. The graph contains semantics, concepts, annotations and relationships used in the domain. VUE exports the graph in Resource Description Framework (RDF), which is the base construction language of an OWL-DL ontology.
Although other flavours of OWL such as “OWL Lite” and “OWL Full” are capable of capturing semantics of nursing processes. The OWL-DL RDF/XML ontology format was chosen for this pilot study because OWL-DL ontologies may be re-used in future tests examining logic consistency and interfacing.
The ontology is constructed in the ontology development platform, Protégé 4.3 (Stanford, 2011) because Protégé is supported by a global community. When the ontologies are completed, an automated agent (OnAGUI) (Charlet, 2015) , ranks semantic similarity across the ontologies.
OnAGUI was chosen for this pilot study above other graph-mapping software such a Cmap (Cañas et al., 2004) for two reasons. First, OnAGUI uses the I-Sub terminological matching algorithm, which calculates a “semantic similarity” decimal between terms across ontologies (Lee, Shah, Sundlass & Musen, 2008). Second, OnAGUI addresses one of the future challenges of semantic matching described by Otero-Cerdeira, et al. (2015). That is, to define tools that are easy to use for non-experts and make what may be a first step toward bringing knowledge acquisition theory into practice.
Graphs and ontologies were also chosen for this study because they have a good “fit” with two theories, which are the foundations of the study’s methodology. That is, Benner’s observation (Benner, 1983) that “knowledge is embedded in practice” and Minsky’s (Minsky, 1974) knowledge acquisition “frames” theory
Benner’s observations on knowledge
Patricia Benner (Benner, 1983) observed that nursing knowledge is embedded in practice. Obviously, it is impractical to interview a front-line nurse while he/she undertakes every step in a process to elicit knowledge. However, the act of constructing a node-to-arc graph prompts nurses to think about their positions in the process domain. As nurses construct a graph, they place themselves in the process domain and mentally “walk through it.” In doing so, the process of constructing a graph may elicit accurate tacit information.
Frames theory
Marvin Minsky’s (Minsky, 1974) frames theory of knowledge acquisition underpins the structure and operation of ontologies. Minsky suggested that domain experts such as front-line nurses store tacit knowledge as cognitive “frames,” which are a “snapshot” or abstract of a past process.
Frames, like slides in a cognitive carousel projector, may be retrieved by the front-line nurse, who when presented with a new situation, compares and is guided in the new situation by the retrieved frame. Differences between the retrieved frame and the new situation modify the original frame for future use.
The Methodology in Detail
The preliminary stage
The purpose of the preliminary stage is to select and educate participants about knowledge acquisition. Participants attended a one-hour tutorial explaining the basics of the pilot study including aspects of knowledge acquisition, graphs and the VUE graphing software.
Participants
Purposive samples of four nurse domain experts (the participants) from different acute nursing specialties were selected. Nielsen (1994) recommended for an initial design science study a sample of not more than five people because he observed there is no point continuing with a large sample if there is a possibility of an inherent problem in the software being studied. The nurse domain experts were chosen to represent a broad spectrum of nursing expertise across emergency, transitional care, administrative and surgical specialties in one Australian hospital. The three selection criteria were:
- Participants have a minimum of 15 years nursing experience in their particular specialties
- Participants are currently working in their specialties
- Participants expressed an interest in knowledge acquisition techniques but have no working knowledge of it.
VUE tutorial
VUE software was loaded onto computers and demonstrated by the researcher. The two-hour knowledge acquisition tutorial included two handouts. The first was a data visualisation handout (Tufts, 2016b) and the second an introduction to the VUE software (Tufts, 2016a). Participants were asked to picture themselves in their process environment and consider concepts they interact with and their relationships to the concepts. Participants were informed that concepts in the process domain could be “concrete” things such as medications or health workers or abstract concepts such as “nursing care.”p>
The data capture stage
The data capture stage proceeded in the following three steps:
- The participants constructed graphs from a supplied “base-line” graph using VUE software
- Graphs were checked and de-personalized by the researcher
- Graphs were checked by their authors and changed if necessary.
The “base-line” graph
An identical base-line graph (Figure 2) was given to each participant. The graph was a common “starting point,” which contained five concepts, that is, three “nursing roles,” a doctor and patient. The nursing roles were derived from the Nursing Role Effectiveness Model (NREM) (Doran et al., 2006) The roles are:
- Independent: roles in which nurses act independently
- Interdependent: roles in which nurses consult with allied health
- Dependent: roles in which nurses follow a doctor’s orders.
A doctor and patient concept was included because these entities would naturally occur in a nursing process domain, and consequently, they are not included in the final semantic ranking.
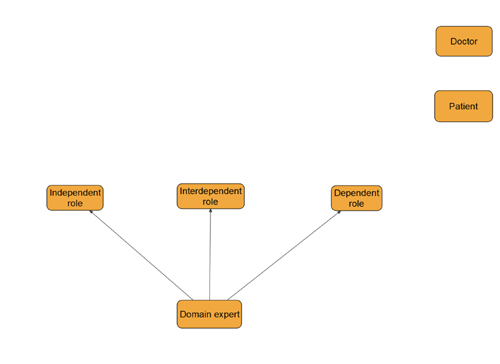
Figure 2: The base-line graph
Participants created their own concepts, placed labels and annotations that explained the concepts, and connected relationship arcs from their concepts to the five supplied base-line concepts.
The ontology construction stage
The purpose of this stage was to construct OWL-DL ontologies from graphs. The stage proceeded in three steps:
- The researcher exported participants’ graphs as RDF into the Protégé 4.3 ontology development platform
- The researcher used Protégé 4.3 to construct OWL-DL ontologies
- The researcher concluded a manual “double-check” of semantics between graphs and ontologies.
Exporting four graphs into Protégé
Graphs can be exported as RDF from VUE into Protégé 4.3. With some manual checking by the researcher, Protégé 4.3 produces OWL-DL ontologies equivalent to the participants’ graphs. Each node-to-arc graph was checked manually against its equivalent in the ontology to detect any semantic errors that may have occurred as a result of the graphs being exported into Protégé.
Ontology validation
One of the primary goals of ontology evaluation is the identification of anomalies. The four ontologies in this study were internally validated three ways. First, the ontologies were checked against Rector et al’s. (2004) set of common errors made by developers during the ontology modeling process, which are:
- Failure to make all information explicit
- Use of universal rather than existential restrictions as the default
- Open world reasoning
- The “flow-on” effect of range and domain constraints.
Second, the ontologies were compared with the source of data (graphs) used to construct the domains (Poveda Villalon, Suárez-Figueroa, & Gómez-Pérez, 2010). Finally, the completed ontologies were parsed through Poveda-Villalón et al’s on-line ‘OOPS!’ validator (Poveda-Villalón, Suárez-Figueroa, & Gómez-Pérez, 2012).
External validation against a “gold standard” process domain ontology was deemed almost impossible because the participant’s ontologies were “one-off” and represented the participant’s perception of the domain.
Pattern of NREM roles in each graph
The number of arcs from each NREM role to participant’s concepts may represent the overall role “autonomy” perceived by the participant.
Pattern of the number of clusters in each graph
Clusters in the context of this study are defined as four or more concepts surrounding a central concept. The numbers of clusters in the graph were counted to indicate possible areas of increased nursing responsibility.
Semantic similarity ranking across ontologies using OnAGUI
OnAGUI compares labels placed on concepts by participants and ranks the semantic similarity to terms in other ontologies. To stop OnAGUI ranking terms that are obviously dissimilar the algorithm was set to reject term matches lower than 0.70. The threshold of 0.70 was chosen because it is slightly above Stoilos, Stamou, and Kollias (2005) and slightly below Euzenat and Le Duc (2012)’s experimental thresholds.
OnAGUI has the following output:
- Terms which ranked above 0.70 across all four ontologies
- Identical terms
Results
The results section commences by presenting each graph in turn with NREM and cluster patterns in each graph. Following the graphs are tables displaying the semantic evaluation, which consists of the ranking of terms edit distance between the ontologies.
The node-to-arc graphs
The following Figures 3 to 6 are the four graphs drawn by the front-line nurses in VUE. The nurses had no previous knowledge of semantic networks, graphs or knowledge acquisition before they drew the graphs

Figure 3: Transitional nurse graph showing links to NREM roles
The transitional nursing process domain
Figure 3 depicts the transitional care process domain graph. The transitional care participant identified five arcs from the independent role, one arc from the dependent role, and one arc from the interdependent role. Clusters appear around concepts denoted as “allied health,” “case conference,” “patient” and “external agencies.”

Figure 4: Surgical nurse graph showing links to NREM roles
The surgical nursing process domain
Figure 4 is the surgical process domain graph. The surgical participant identified six arcs from the independent role, one arc from the dependent role, and one arc from the interdependent role. In comparison to the previous transitional care and following administrative and triage graphs, this surgical graph contains the most arcs radiating from the independent role and the most clusters. Five clusters in this graph are: “computers,” “medication administration,” “documentation,” “patient” and “referrals to allied health.”
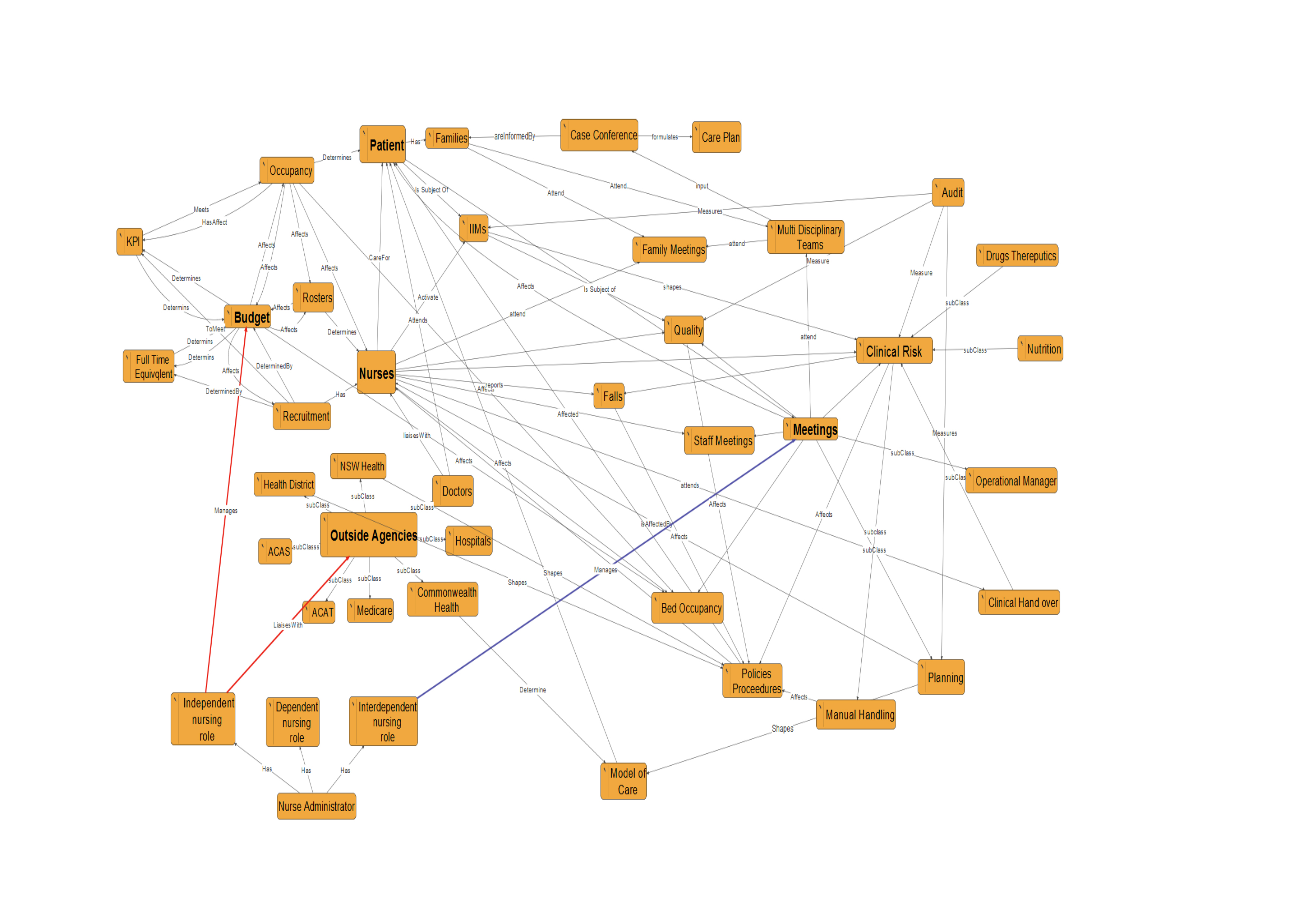
Figure 5: Administrative nurse graph showing links to NREM roles
The administrative nursing process domain
Figure 5 is the administrative process domain graph. The administrative participant identified two arcs from the independent role, no arcs from the dependent role, and one arc from the interdependent role. Five clusters can be seen in the graph: “budget,” “nurses,” “patient,” “outside agencies” and “meetings.”
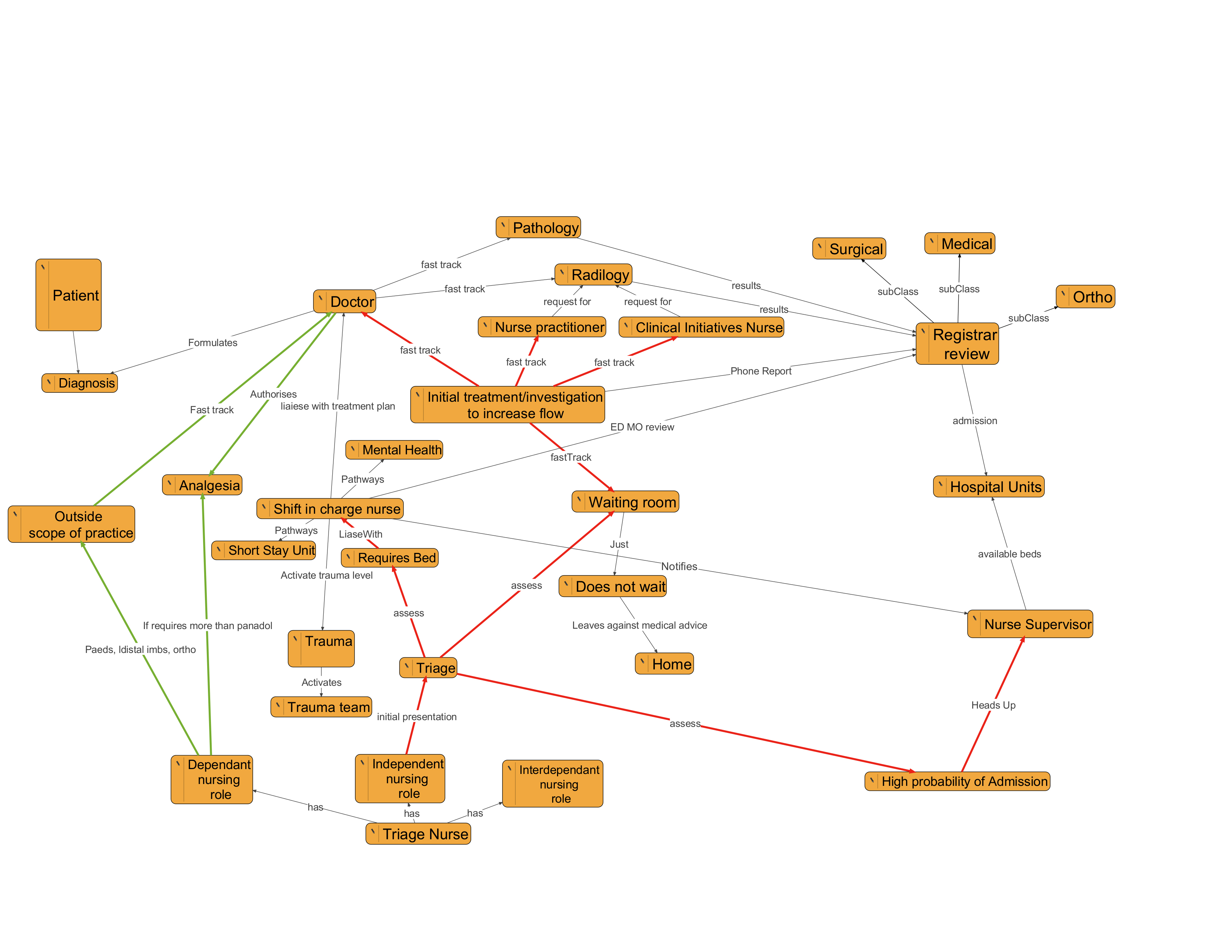
Figure 6: Triage nurse graph showing links to NREM roles
The triage nursing process domain
Figure 6 is the graph of the triage process domain. The participant identified one arc from the independent role and two arcs from the dependent role. There are no interdependent roles marked. This graph is different from the previous three graphs in that the participant identified no clusters. Also, many arcs terminate at other staff members such as doctor, nurse practitioner, shift in-charge nurse and nurse supervisor. The patient was placed off to the side of the graph because “the patient concept would encompass the entire graph,” as commented by the participant, and the graph would lose readability. It is beyond the scope of the thesis to theorize on the nurse’s perception of the patient’s position in the graph.
The ranking of semantic similarity
Tables 2 to 7 contain results of the ranking of terms, with two ontologies per table. One term from each ontology appears in the first two columns and the last column contains the I-Sub semantic similarity number for each term match. As mentioned previously, a ‘1’ represents an exact match and the cut-off threshold for I-Sub was set at 0.7.
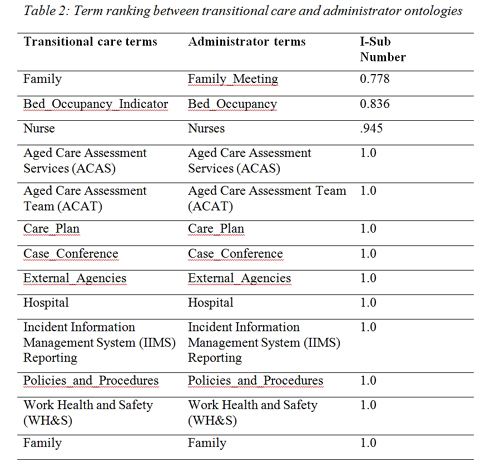
Table 2: Term ranking between transitional care and administrator ontologies
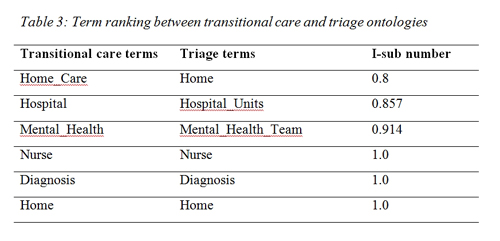
Table 3: Term ranking between transitional care and triage ontologies
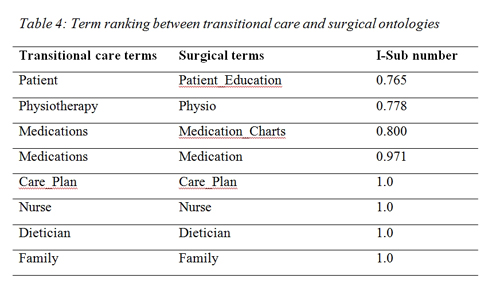
Table 4: Term ranking between transitional care and surgical ontologies
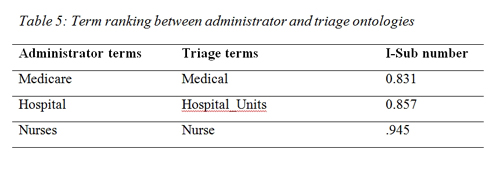
Table 5: Term ranking between administrator and triage ontologies
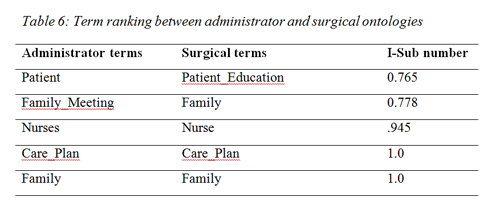
Table 6: Term ranking between administrator and surgical ontologies
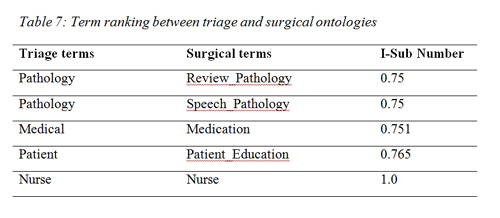
Table 7: Term ranking between triage and surgical ontologies
OnAGUI found no identical terms occurred in all four ontologies. However, three identical terms occurred in three ontologies, these were:
- Care plan used in surgical, administration, transitional care
- Family used in surgical, administration, transitional care
- Nurse used in transitional care, triage, and surgical.
Discussion
Although the original intention of the study was to acquire process domain semantics using ontologies, their complexity added an enormous overhead for the participants in the study. However, node-to-arc graphs provided a “work-around” visual representation, which enabled participants to construct their process domains. The implication being that graphs may provide insights into “real world” nursing processes and relationships that may be used to construct an ontology. The following discussion pertains to participants’ process domain graphs and semantic similarity of terms in ontologies.
The transitional care nurse process domain graph
As shown in Figure 3, the “transitional care” concept is divided into two sections, “community in own home” and “residential in facility.” Linked concepts can be seen to reach beyond transitional care into the wider community and surrounding hospitals. In this way, concepts extending to the patient’s home and the wider community may suggest a “horizontal” care structure. That is, patient pathways transcend organizational boundaries and connect community-based stakeholders. On the other hand, there is evidence of a more traditional vertical “medical model” structure. This is the only graph, out of the four graphs, where both horizontal and vertical models seem to exist.
The surgical nurse process domain graph
The surgical nurse graph in Figure 4 has the most number of clusters (5) out of the four graphs. The surgical nurse is connected to all clusters to which the patient is connected. This may suggest that the surgical nurse is involved in the majority (if not all) aspects of patient care.
The “medication administration” and “patient” clusters contain some connected concepts that may be termed “hidden’ processes,” which are elusive and not normally captured in other studies. Examples of hidden processes in this surgical graph are:
- Checking dangerous drugs (DDs)
- Finding keys to the drug room
- Other nurses to help check drugs
- Answering phones
- Supervising student nurses
- Making beds.
It is possible that time may be taken from face-to-face patient care when dealing with the many unrecorded hidden processes that are connected to the medication administration cluster and the computer cluster.
The surgical nurse participant had the most independent roles out of the four graphs, six in total. The sole dependent role is connected to the doctor who prescribes medication. This may suggest that the surgical nurse is mostly autonomous and is concerned with almost every aspect involved with direct patient care.
The administrative nurse graph
The administrative nurse graph in Figure 5 has the most interlinked concepts of the four graphs. Many interlinked concepts may suggest complex interactions between the budget, nursing staff and the various meetings. A couple of observations can be made from the graph:
- The graph shows that the administrative nurse has no direct connection to the nursing staff or the patient
- Indirect connections to staff and patients may occur as a result of outcomes of meetings and the regulation of the budget.
Nurses are connected to the budget through rosters, recruitment and bed occupancy concepts. Patients are connected to the budget concept through a bed occupancy concept. It is clear from the administrative graph that the major drivers of the graph are the budget and meeting concepts. The budget may be influenced by bed occupancy numbers, which is most likely a primary source of income for the facility. The administrative participant expressed surprise about the indirect arcs in the graph.
The administrative nurse graph contains no dependent roles and may suggest that the nurse administrator is probably autonomous with regard to decisions concerning the budget, implementation of meeting outcomes and external agency liaison. It is interesting that the administrator does not have a “higher nurse authority to which to refer. Instead, there are state and commonwealth bodies that dictate care models and policy. This may also suggest a high degree of autonomy.
The triage nurse process domain graph
Compared to the other three graphs, the triage graph is the only graph without “clusters.” There are no clusters because the triage participant’s arcs either terminate at a person who effects the actual care, or a location in the emergency department (ED). The pattern of arcs terminating at other people or locations in the ED suggests an underlying strict procedural structure that may govern the placement and ranking of patients. The “clusterless” graph structure may also facilitate care as quickly as possible—as suggested by the arcs labelled “fast track” and “assess.” These arcs terminate at a concept of someone or something that continues patient care.
The graph may suggest patient “load sharing,” through which patients are allocated equally to care providers. Concepts connected to a concept called “initial treatment/investigation to increase flow” may suggest patient load sharing. This concept may increase patient flow through the process domain by distributing the patient load between the doctor, clinical initiative nurse and nurse practitioner concepts.
The “shift in charge nurse” concept is a central figure in the graph that is connected to mental health, short stay unit, trauma, doctor and supervisor concepts. This may suggest that the shift in charge nurse has an “overall view” of triage and may escalate patient care if the need arises. The shift in charge nurse concept may act as a “buffer” between the triage nurse and the rest of the ED. This may indicate a fair degree of isolation of the triage nurse from the wider ED and hospital. This “isolation” may have been illustrated by the textual ranking agent OnAGUI, which identified triage as having the most exclusive language.
The triage participant did not add any interdependent roles to the graph. The lack of these arcs may suggest that the triage nurse has little interaction with allied health. On the other hand, independent roles are dominant in the graph and show clear pathways to concepts that further the care of the patient.
Dependent roles are minimal for the triage nurse. The only two dependent roles are “analgesia” (because the triage nurse requires a doctor to fill out a medication chart) and a larger concept called “outside the scope of practice,” which is everything else that requires a doctor’s order.
The OnAGUI textual ranking
The results in tables 2-7 may be viewed as trivial “stepping-stones” to a future, more complex, study. This pilot study ranked simple semantic string similarity between ontologies; it was not evaluating the matching algorithm’s performance using classic metrics, such as precision and recall.
The ontology matcher for this project had to fulfil the following criteria:
- An uncluttered, easy-to-use graphic interface
- Display strings from each ontology
- Rank strings from ontologies with Levenchine or I-Sub algorithms.
An ontology mapping tool meeting the above criteria was elusive.
However, OnAGUI fulfilled the preceding requirements and ranked terms across four ontologies to ascertain identical terms. Our thinking was that if enough identical terms exist across the ontologies, a single “global” vocabulary of terms may emerge. Also, if identical terms are identified in different ontologies, these may be used to connect ontologies together.
OnAGUI found the number of identical terms across the four ontologies was minimal. The agent found that there were not enough identical terms to construct one overarching vocabulary. Only three terms were common across the four ontologies – “care plan,” “family,” and “nurse.”. That is, three terms out of 145 terms ranked by OnAGUI were used in all four ontologies, on average, 78.12% exclusive language.
The lack of similar terms may suggest “siloing.” The silo effect refers to a lack of information flowing between nursing specialities. Siloing is an analogy describing the effect of silos on a farm in which the silos prevent different grains from mixing. In healthcare, the silo effect may limit interactions between nursing specialities, leading to reduced patient care. OnAGUI may identify silos that may be removed to foster innovation and increase productivity by unlocking the information needed for collaboration.
Transitional care displayed 11 identical terms with the administrator, four identical terms with surgical, and three with triage. Transitional care’s relatively high number of identical terms with other ontologies may reinforce the notion of transitional care having a “horizontal” care structure component that expands out into the wider community and other nursing process domains (as discussed earlier).
Conversely, the triage ontology table had the least number of identical terms when compared with other ontologies. Triage had no common terms with the administrator, one common term with surgical and three with transitional care. An explanation for the lack of common terms may be due to the triage nurse not having direct contact with the wider hospital as previously discussed.
Significance
This pilot study provides one way of overcoming contemporary limitations of ontology construction. Prior to this study, nurses have not had direct input into the construction of complex ontologies. Graphs in nursing are innovative because the approach developed in this study may facilitate a clearer and more faithful representation of the process domain. Finding this representation has been elusive. More importantly, the approach may be a conduit to industries other than nursing to provide evidence of nursing’s contribution to patient care; all of which may improve understanding between nurses, policy makers and computer science researchers and ultimately translate into improved patient outcomes.
Benefits and contribution to nursing informatics
Overall, semantic technology provides one more “tool” in the informatics nurse’s toolbox. Clark and Lang (1992), summed up the use of data acquisition saying: “If you can’t name it (identify the process), you can’t control it, finance it, research it, teach it or put it into public policy” (p154).
This study is a first step in using semantic technology to capture a “snapshot” of first-hand nursing processes that may be analysed by humans and computers. The following are some possible benefits from the use of semantic technologies used in this study.
Graphs detailed in this paper may be used in hospitals:
- Persistent organizational memory: graphs are “consumable” knowledge that can be stored; processes are not lost if a key member leaves the organization
- Process modulation: graphs may be used to add or delete redundant processes, thus improving patient outcomes and productivity
- Identification of semantics: semantics may be identified for use in the construction of nursing minimum data sets and electronic health records
- Teaching tool: graphs may be useful for undergraduate studies and as evidence to show non-clinicians where resources/money could be better placed
- Process concordance: nurses in one unit may each construct a graph to see if “everyone is on the same page.” Consequently, graphs may be used to triangulate common processes across the unit.
Participants agreed that by constructing their process domain in VUE, they gained a better insight into their processes.
Ontologies are the machine-readable version of the graph and may have the following benefits:
- Ontologies used in this study can deduce inferences: for example, patients in a process domain may have multiple acuity scores. An ontology can infer resources according to the scores
- Ontologies can be linked to other ontologies to add knowledge: our process domain can be linked to the ICD-10 and/or SNOMED-CT ontologies to infer patient codes
- Ontologies are machine-readable: a variation of the semantic similarity agent used in this study may form the basis of automated auditing of a hospital unit.
Conclusion
The motivation for this pilot study was to find a way for nurses, who are not experts in knowledge acquisition or ontologies, to impart process semantics that could be used to fill the lack of tacit semantics in other areas of nursing. Underpinning this study is the notion that process semantics will be more “accurate” if they are sourced directly from the nurses who use them daily.
The study found that simple graphing software such as VUE is a useful “stand-alone” knowledge acquisition tool for the visualization of semantics forming the basis of the process domain from the nurse’s perspective. The nurse’s graphs were used to construct OWL-DL ontologies. It followed that semantics in ontologies, from the original nurse’s graphs, can be evaluated by an automated agent and may produce useful information.
An automated agent ranked semantic similarity across the four ontologies representing different nursing disciplines and found almost exclusive language being used in each ontology. This may suggest “siloing.” In healthcare, the silo effect may limit interactions between nursing disciplines, leading to reduced patient care.
The study ventured into unexplored territory between nursing and semantic technology and is one of the first nursing studies to draw upon techniques from both realms. On one side, nursing tools-of-trade for this study were semantics and nursing frameworks. On the other, graphs and ontology provided the knowledge acquisition frameworks. Both are a means to an end, that is, to achieve the best possible patient outcomes.
Appendix A: Basic Node-to-Arc Graphs
On first glance, node-to-arc graphs look like a concept map. They detail a nursing process domain by linking nodes (concepts), their relationships (arcs) labels of concepts and annotations describing what things do (Noy & McGuinness, 2001). Concepts in a nursing process domain are typically patients, nurses and doctors, or even abstract concepts such as “nursing care.” Graphs are designed to be linked on the internet using their underlying Resource Description Framework (RDF), the language of ontologies. A single graph represents one relationship between two concepts.
Figure A.1 illustrates a simple graph that displays the relationship between two concepts: “Bob and Alice.”
Figure A.1: The ‘Bob Knows Alice’ graph
In reality, graphs contain detailed descriptive semantics conforming to World Wide Web Consortium (W3C) specifications. For example, Bob and Alice’s relationship, called “knows,” is linked to a W3C specification (SemanticWeb, 2013), which describes the parameters of “knows.”
Appendix B: What Is an Ontology?
An ontology is a computer-readable document which contains a sharable, agreed upon, formal representation of knowledge for a specific domain of interest, which in our case is the nursing process domain. Ontologies are a mixture of database, concept map, “real world” model and logical inference engine.
This study uses “ontology” in its design science context and adopts the most commonly accepted definition proposed by Gruber (2004): “a formal, explicit specification of a shared conceptualization.” This meansan ontology may define common, agreed-upon and sharable semantics that may describe concepts and relationships. In doing so, an ontology “paints a semantic picture” of some “domain of interest” that computers can read and analyze. A domain of interest is a “snapshot” of some section of the “real world,” which in our case is the nursing process domain (what nurses do).
Unfortunately, ontologies are generally employed as a simple database and their real world modelling functionality is seldom realized.
Little (2009) argued that a major theoretical problem that informatics research must address is that of providing an accurate, comprehensive and consistent description of our world that computers can understand. Dr. Little observed computerized ontologies often depict a limited knowledge of the more traditional sense of ontology; that is, the study of being and existence. He noted computer ontologies are designed to be computationally tractable rather than grounded in classical philosophical aspects of ontology.
A OWL-DL ontology used in this study makes it possible for software “agents” to automatically compute logical inferences and check for inconsistencies in our domain of interest.
Acknowledgements
I wish to express my thanks to my supervisors, Associate Professor Liza Heslop for her guidance and encouragement throughout the course of the Ph.D., and Dr. Sai Lu for her assistance relating to the development of the thesis and guidance with submissions to various conventions.
Funding
This work is part of my Ph.D., which was supported by Victoria University, College of Health and Biomedicine, Nursing & Midwifery, Melbourne Australia. I gratefully acknowledge my full-time, three-year faculty scholarship and two travel grants.
Citation: Shields, P. (2018). Capturing and evaluating process semantics from front-line nurses: A pilot study. Online Journal of Nursing Informatics (OJNI), 22(1), Available at http://www.himss.org/ojni
The views and opinions expressed in this blog or by commenters are those of the author and do not necessarily reflect the official policy or position of HIMSS or its affiliates.
Online Journal of Nursing Informatics
Powered by the HIMSS Foundation and the HIMSS Nursing Informatics Community, the Online Journal of Nursing Informatics is a free, international, peer reviewed publication that is published three times a year and supports all functional areas of nursing informatics.
Author Bio
Philip John Shields, Ph.D., R.N., received a first class honours degree from Latrobe University, Melbourne, Australia, while undertaking a nursing graduate year at Wodonga Hospital, Victoria, in 2009. He received a full-time Ph.D. scholarship from Victoria University, College of Health and Biomedicine, School of Nursing and Midwifery, in Melbourne and my Ph.D. was conferred in 2017. Dr. Shields is researching inferred nursing knowledge using OWL-DL ontologies at the Centre for Health Research and Education in Melbourne, Australia.
In his 35-year working life, he has been employed in two contradictory roles: the first, electronics/IT, and the second, health. In his health career, he was a rural/remote paramedic in outback Australia and a front-line nurse in a metropolitan hospital.
In electronics/IT, he prototyped military robotic technology and communications using various programming languages. The two parts of his working life have recently merged with the advent of clinical informatics, which has allowed him to explore and hopefully bridge uncharted ground between the two worlds.
References
Anand, S., & Verma, A. (2010). Development of Ontology for Smart Hospital and Implementation using UML and RDF. International Journal of Computer Science Issues, 7(5), 1694-0814.
Becker, M., Heine, C., Herrler, R., & Krempels, K. H. (2003). OntHoS—an Ontology for Hospital Scenarios. In A. Moreno & J. Nealon (Eds.), Applications of Software Agent Technology in the Health Care Domain (pp. 87-103). Basel: Birkhauser Verlag.
Benner, P. (1983). Uncovering the knowledge embedded in clinical practice. The Journal of Nursing Scholarship, 15(2), 36-41.
Burnes Bolton, L., Donaldson, N. E., Rutledge, D. N., Bennett, C., & Brown, D. S. (2007). The Impact of Nursing Interventions: Overview of Effective Interventions, Outcomes, Measures, and Priorities for Future Research. Medical Care Research and Review, 64(2), 123-143.
Butler, M., Treacy, M., Scott, A., Hyde, A., Mac Neela, P., Irving, K., . . . Drennan, J. (2006). Towards a nursing minimum data set for Ireland: making Irish nursing visible. Journal of Advanced Nursing, 55(3), 364-375.
Cañas, A. J., Hill, G., Carff, R., Suri, N., Lott, J., Eskridge, T., et al. (2004). CmapTools: A knowledge modeling and sharing environment. In A. J. Cañas, J. D. Novak & F. M. González (Eds.), Concept maps: Theory, methodology, technology. Proceedings of the first international conference on concept mapping (Vol. I, pp. 125-133). Pamplona, Spain: Universidad Pública de Navarr
Charlet, J. (2015). OnAGUI ontology matcher. from https://sourceforge.net/projects/onagui/
Clark, J., & Lang, N. (1992). Nursing's next advance: An internal classification for nursing practice. International Nursing Review, 39(4), 109-112.
Daniyal, A., Abidi, S. R., & Abidi, S. S. R. (2009). Computerizing clinical pathways: ontology-based modeling and execution. Studies in Health Technology and Informatics, 150, 643-647.
Din, M. A., Abidi, S., & Jafarpour, B. (2010). Ontology based modeling and execution of nursing care plans and practice guidelines. Studies in Health Technology and Informatics 160(Pt 2), 1104-1108.
Doran, D., Harrison., Laschinger, H., Hirdes, J., Rukholm, E., Sidani, S., . . . Cranley, L. (2006). Relationship between nursing interventions and outcome achievement in acute care settings. Research in Nursing and Health, 29(1), 61-70. doi: 10.1002/nur.20110
Euzenat, J., & Le Duc, C. (2012). Methodological guidelines for matching ontologies Ontology engineering in a networked world (p. 257-278), Springer-Verlag Berlin Heidelberg .
Gruber, T. (2004). Every Ontology is a Treaty. Interview for Semantic Web and Information Systems SIG of the Association for Information Systems. Semantic Web and Information Systems 1(3), 1-5.
Hurley, K. F., & Abidi, S. S. R. (2007). Ontology engineering to model clinical pathways: Towards the computerization and execution of clinical pathways. Paper presented at the Twentieth IEEE International Symposium on computer-based medical systems, June 20 - 22, Maribor, Slovenia.
Institute of Medicine. (2011). IOM Report on the Future of Nursing: Leading Change, Advancing Health. Medical-Surgical Matters, 20(1), 3-3.
Lee, W. N., Shah, N., Sundlass, K., & Musen, M. (2008). Comparison of ontology-based semantic-similarity measures. Paper presented at the American Medical Informatics Association annual symposium, New York.
Little, E. (2009). A proposed methodology for the development of application based formal ontologies. Buffalo, USA: Center for Multisource In formation Fusion.
Minsky, M. (1974). A framework for representing knowledge. DSpace@MIT. Retrieved 19 September, 2011, from http://dspace.mit.edu/handle/1721.1/6089
Needleman, J., Kurtzman, E. T., & Kizer, K. W. (2007). Performance Measurement of Nursing Care: State of the Science and the Current Consensus. Medical Care Research and Review, 64(2), 10-43.
Nielsen, J. (1994). Usability engineering (Vol. 1). Cambridge MA USA: AP Professional.
Noy, N. F., & McGuinness, D. L. (2001). Ontology development 101: A guide to creating your first ontology. Stanford Il USA: Stanford knowledge systems laboratory.
Otero-Cerdeira, L., Rodríguez-Martínez, F. J., & Gómez-Rodríguez, A. (2015). Ontology matching: A literature review. Expert Systems with Applications, 42(2), 949-971.
Peffers, K., Tuunanen, T., Gengler, C. E., Rossi, M., Hui, W., Virtanen, V., & Bragge, J. (2006). The design science research process: a model for producing and presenting information systems research. Paper presented at the Proceedings of the first International Conference on Design Science Research in Information systems and Technology, February 24-25, Claremont, California.
Poveda-Villalón, M., Suárez-Figueroa, M. C., & Gómez-Pérez, A. (2012). Did you validate your ontology? OOPS! Paper presented at the Extended Semantic Web Conference. Retrieved from http://www.upm.es/sfs/Rectorado/Vicerrectorado%20de%20Investigacion/Ofi…
Poveda Villalon, M., Suárez-Figueroa, M. C., & Gómez-Pérez, A. (2010). A double classification of common pitfalls in ontologies Retrieved from http://oa.upm.es/5413/1/A_DOUBLE_CLASSIFICATION_OF_COMMON_PITFALLS_IN_O….
Rector, A., Drummond, N., Horridge, M., Rogers, J., Knublauch, H., Stevens, R., . . . Wroe, C. (2004). OWL pizzas: Practical experience of teaching OWL-DL: Common errors & common patterns. Paper presented at the International Conference on Knowledge Engineering and Knowledge Management, October 5-8, Whittlebury Hall, UK.
Savitz, L. A., Jones, C. B., & Bernard, S. (2010). Quality Indicators Sensitive to Nurse Staffing in Acute Care Settings. Advances in Patient Safety, 4, 375-385. Retrieved 12 May, 2011, from http://www.ahrq.gov/downloads/pub/advances/vol4/Savitz.pdf
SemanticWeb (2013). FOAF.The Friend of a Friend Vocabulary. Retrieved 24 October, 2013, from http://semanticweb.org/wiki/FOAF.html
Stanford. (2011). Protege ontology editor. Retrieved 12 June, 2011, from http://protege.stanford.edu/download/protege/4.3/installanywhere/Web_Installers/
Stoilos, G., Stamou, G., & Kollias, S. (2005). A String Metric for Ontology Alignment. In Y. Gil, E. Motta, V. R. Benjamins & M. Musen (Eds.), The Semantic Web – ISWC 2005 (Vol. 3729, pp. 624-637): Springer Berlin Heidelberg.
Tufts. (2016a). Introduction to VUE. Retrieved 20 August, 2016, from vue.tufts.edu/content/VUE2%20handout.pdf
Tufts. (2016b). Things you should know about data Visualization II. Retrieved 23 August, 2015, from http://www.educause.edu/ir/library/pdf/ELI7052.pdf
Tufts. (2016c). VUE. Visual Understanding Environment. Retrieved 20 June 2016, 2015, from vue.tufts.edu/download/index.cfm
Ye, Y., Jiang, Z., Diao, X., Yang, D., & Du, G. (2009). An ontology-based hierarchical semantic modeling approach to clinical pathway workflows. Computers in Biology and Medicine, 39(8), 722-732.
Source:
Online Journal of Nursing Informatics: Volume 22, Winter 2018
Published on
February 27, 2018