Patient Access
Davies Award of Excellence

Executive Summary
In 2016, Children’s Hospital of Orange County (CHOC) was awarded the HIMSS Davies Award. One of the award-winning case studies focused on using embedded, evidence-based care guidelines to control pediatric asthma and an alert system that triggered when patients were about to be discharged before a home management plan was created. CHOC drove down the average length of stay for pediatric asthma patients from 2.14 days to 1.72 days. Pediatric asthma readmissions within 30 days also fell from an average of 1.7 per quarter to 0.7 per quarter. To sustain and expand on this work, in 2017 the organization decided to re-focus on the pediatric condition registries which had first been installed in 2015. It organized and stabilized the number of primary care patients who received an pediatric asthma action plan (AAP) and asthma control test (ACT) resulting in lower emergency room visits and inpatient hospital admissions. The process re-design was driven by analytical data which was reviewed on a monthly basis for transparency into how providers were performing against their value measurements. The utilization of a population health platform empowered the team to take disparate sources of data (different electronic health records, claims, labs, pharmacy data, etc., and transform the data in to meaningful, useful information and integrate the required documentation into the EHR. In total, CHOC built six ambulatory guidelines of care into their EMR, one of which was asthma, leading to the overall improvement in the ambulatory care of pediatric asthmatics. The results included:
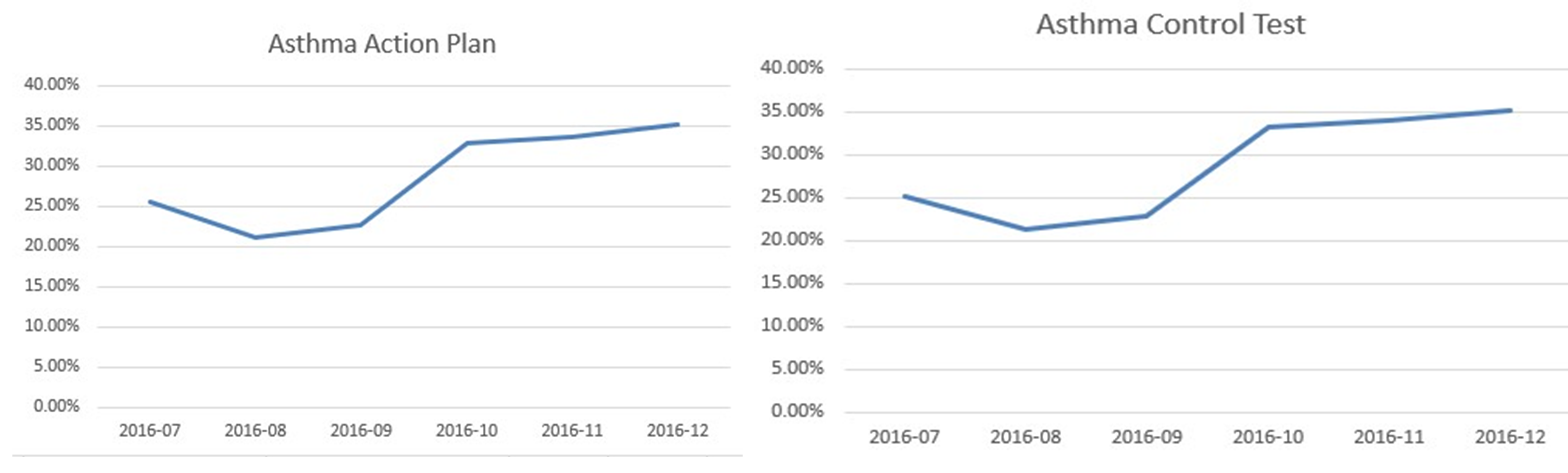
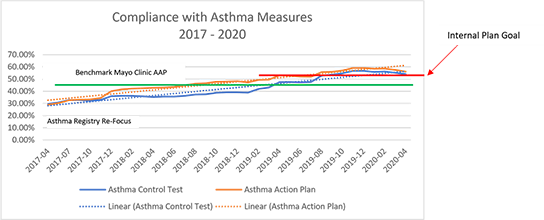
- In December 2019, ~59% of primary care patients received the pediatric asthma action plan—up from 28.89% in April 2017.
- In December 2019, 57% of primary care patients received the asthma control test—up from 29.61% in April 2017.
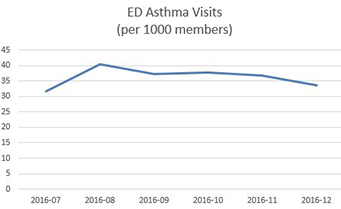
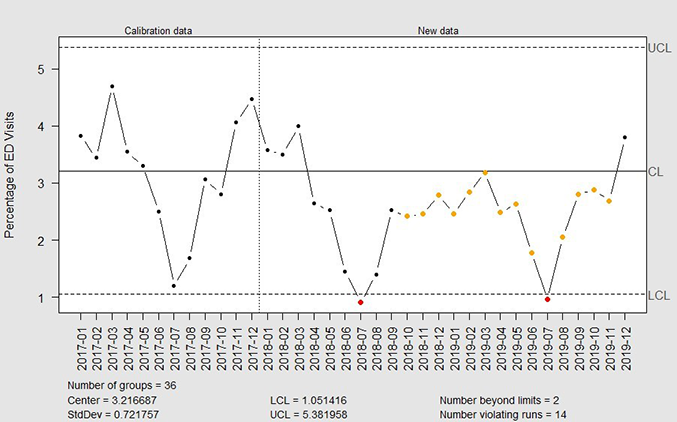
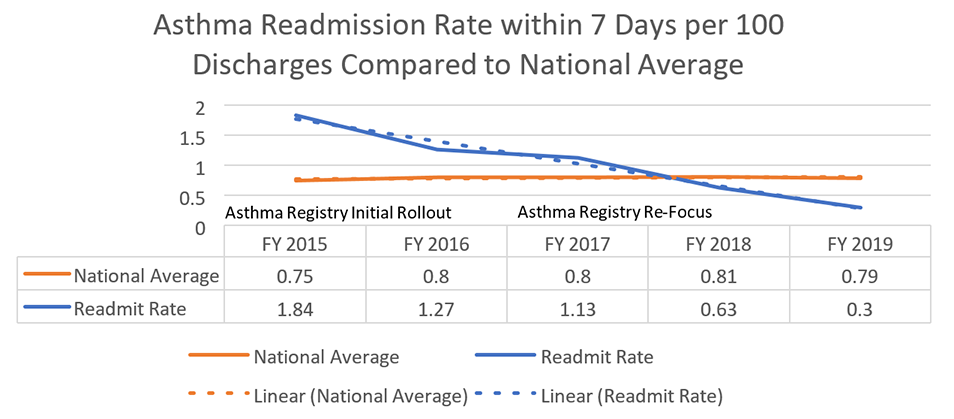
- Patients being seen in the emergency department (ED) for asthma decreased, as well as the readmission rate within seven days of discharge per 100 discharges decreased from 1.84 to 0.3.
The key difference in this case study as compared to the one in 2016 is the work to improve the ambulatory care aspect, as well as continued work in the Breathmobile™ which is the only mobile asthma clinic serving preschool and school-aged kids in Orange County.
Lessons learned include:
The primary and most important take away is to first manage the care of the patients who show up for treatment—and then create an ambulatory plan of care that prevents them from requiring emergent care or hospital admission.
- When choosing registries for implementation, determine which diseases are most prominent in your population.
- Identify which of these diseases lead to increased morbidity, mortality or overall healthcare utilization.
- Understand which of these diseases have well established care guidelines.
- Target disease groups that have willing physicians to partner with on disease registry development.
- Patient and family education, access to care, overcoming social determinants of health issues, improving the use of the Asthma Control Test and the Asthma Action Plan are key to preventing pediatric asthma ED visits and readmissions.
- Engaging the community, schools, and resources like the Breathmobile help to prevent ED asthma visits.
- Care managers and school nurses also play a huge role in asthma management.
Source: Children’s Hospital of Orange County
Defining the Clinical Problem and Pre-Implementation Performance
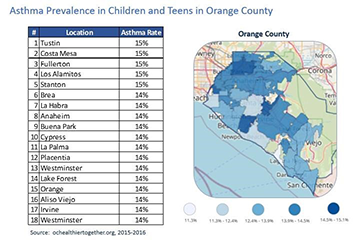
CHOC Medical Group is composed of 54 pediatricians and pediatric nurse practitioners who practice in five clinical sites in Orange County, California. Two sites are on the campus of the Children’s Hospital in the city of Orange, and three sites are in surrounding communities (Santa Ana and Garden Grove) where they support a multicultural population which is entirely Medicaid (MediCal) funded.
The population that CHOC Medical Group serves struggles with barriers such as language discordance, transportation, food and housing insecurity, and various cultural beliefs related to their healthcare. Given the proximity to the U.S./Mexico border, there is a large Latin American population who struggle with immigration issues and in some cases delay/avoid contact with the medical system.
Finally, given CHOCH’s affiliation with the children’s hospital, which is a free-standing tertiary/quaternary children’s hospital, CHOCH primary care clinics support a large volume of hospital graduates with a high degree of complex medical conditions. Preventing emergency room visits and hospital admissions is key to claiming “successful” management of this population. The medical group was struggling to maintain incremental increases in the percentage of pediatric asthmatic patients who had an updated annual AAP and ACT. This was an initiative that the organization and Practice Transformation Network (Southwest PTN—CHOC Children’s and Rady Children’s) had embraced as part of the chronic disease management goal of the Population Health Division’s engagement in the Transforming Clinical Practice Initiative Award CHOC received from the Centers for Medicare and Medicaid Services. CHOC’s subject matter experts identified a wide range of provider/panel completion rates and, as a collective, the group was averaging in the low 30% range. Difficulties with this stemmed from insufficient time for providers to address asthma during routine sick visits and well visits, ineffective capture of patients in the EMR Chronic Disease Registries, inconsistent standards of work for the care team, and variable approaches to compliance from provider to provider and clinic to clinic.
Source: Children’s Hospital of Orange County
The numerators are respectively the patients who received the AAP and ACT, and patients seen in the ED with the diagnosis of asthma. The denominator is the number of patients in the asthma registry with the diagnosis of asthma.
The American Academy of Pediatrics, the Centers for Disease Control, and the National Institutes of Health (NIH) all support the utilization of an Asthma Action Plan and care guidelines specific to pediatric asthma management. Following these guidelines, the chief medical information officer (CMIO) led the asthma registry development with input from an expert panel consisting of asthma experts in pulmonary and allergy, primary care physicians, practice staff, and other pertinent providers. The common goal was to improve compliance and decrease the ED visits and hospital admissions.
The ultimate target to date is to meet and exceed a 54% compliance rate—the benchmark from the American Academy of Pediatrics and Mayo Clinic is 43%.
The organization is currently continuing these efforts and at the time of this writing is working toward The Joint Commission (TJC) Disease Specific Care Pediatric Asthma Certification. This certification will help ensure our program meets clinical performance standards and targeted metrics as well as other compliance standards from TJC.
Designing and Implementing Model Practices and Governance
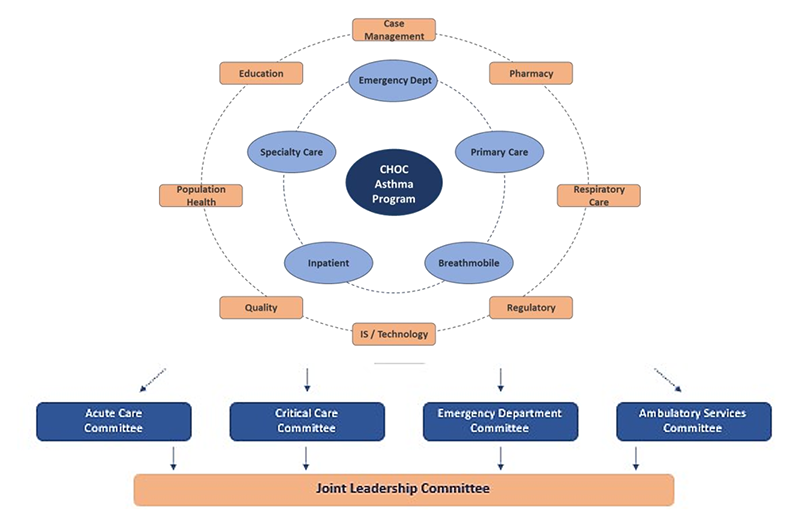
The decision to purchase a population health platform to augment other sources of data such as claims data and the enterprise data warehouse was a turning point in improving our workflows and outcomes. The ability to join the platform supplier as a development partner for pediatric content provided an opportunity to focus on the specific needs of the pediatric population. The purchase of the population health platform was a collaborative decision between the information systems department leadership (the chief medical information officer and the chief information officer at the time), the head of CHOC Health Alliance (independent physician association or IPA) and director over the CHOC population health program, and the vice president of strategic planning, along with other ambulatory and senior leaders. The population health platform, HealtheIntent™ was chosen after a formal RFP process involving several vendors. None of the other population health platforms CHOC evaluated had pediatric content, and the HealtheIntent provider had a long history with our organization of working with CHOC to develop pediatric applications, leading to the choice of HealtheIntent. The multidisciplinary team driving pediatric asthma care is referenced below.
Source: Children’s Hospital of Orange County
Care guidelines supported by the population health management tool which include measures from the asthma registry were embedded in the standard primary care workflow. Processes were developed to create a uniform and consistent standard of work regardless of provider or location and to identify patients with asthma requiring an asthma AAP and ACT.
Learning resources included:
- HealtheRegistries® Help Page
- User Guides for Providers, Office Staff, and Personnel
- Job Aides
- Adoption Strategy—CHOC Learning Plan
- Ex: Pamphlets—Ideal for scattered audiences or as a supplement educational piece
- Ex: Hospital Sessions—Ideal for large group trainings
- Ex: Individual Clinic Visits—Ideal for onboarding new physicians
Enabling Clinical Transformation Through Information and Technology
The foundational component of the CHOC Children’s Population Health program is the creation of a single patient-centered plan of care that can be used by the entire care team across the complete care continuum. Having the actionable data visible at the point of care helps to ensure compliance and outcomes are constantly at the forefront of patient care. The primary office staff prep the asthma charts prior to the visit, the care team medical assistants, licensed vocational nurses, mid-levels, physicians, care managers, school nurses, and Breathmobile staff all have access to the same clinical data.

Source: Children’s Hospital of Orange County
To develop the condition-specific pediatric registries, the team conducted research to determine which diseases were most prevalent in CHOC’s population and which of those diseases led to the most frequent ED visits and hospitalizations. The pediatric asthma registry was created because of the volume and impact this population of patients brings to CHOC. Approximately 13% of CHOC’s capitated, (value-based per member, per month payment system), population has a diagnosis of asthma, and it is the most frequent cause of visits to the ED as 30% of children with asthma visit the ED every year. Asthma is also one of CHOC’s most frequent causes of hospitalization and 5% of children with asthma are hospitalized every year, while 40% miss five or more school days every year from asthma exacerbations. Asthma severity is classified as mild intermittent, moderate, and severe persistent, per NIH guidelines. The team’s recommended care includes assessing an ACT at least once a year and annually updating an AAP specific for that patient. The asthma registry focusses on these two and other measures like appropriate controller meds being given as prescribed.
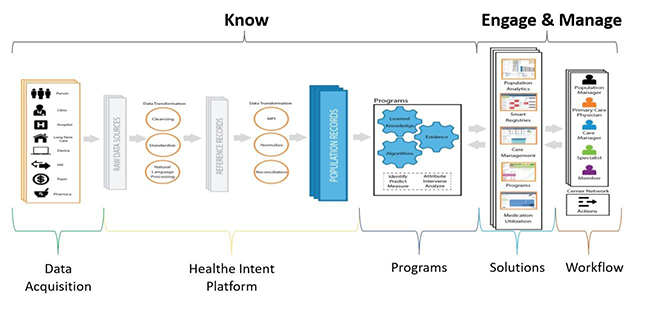
Operationalizing the registries is another key to our success. Prior to the patient visit, the primary office staff have already identified key elements which may need to be addressed and can intervene to raise awareness to the appropriate care team member, including the patient’s family. Running in the background of the EHR is technology that goes beyond just the claims data, and pulls in disease specific clinical data. This data platform allows specific care plan and treatment modalities to be pushed to the provider’s workflow at the point of care. This population health platform is a cloud-based, programmable platform that is vendor-agnostic, which means it can receive data from any EHR, existing health IT system and other data sources, but also pharmacy, eligibility, laboratory and other sources of relevant information. In building the disease specific registries, the first step was to consider the data needs, and then to prioritize the development of the tools. The steps include acquiring the data, normalizing and data transformation, creating the disease specific algorithms, and building specific tools to push the information into the workflow at the point of care as shown in the interface diagram.
Source: Children’s Hospital of Orange County
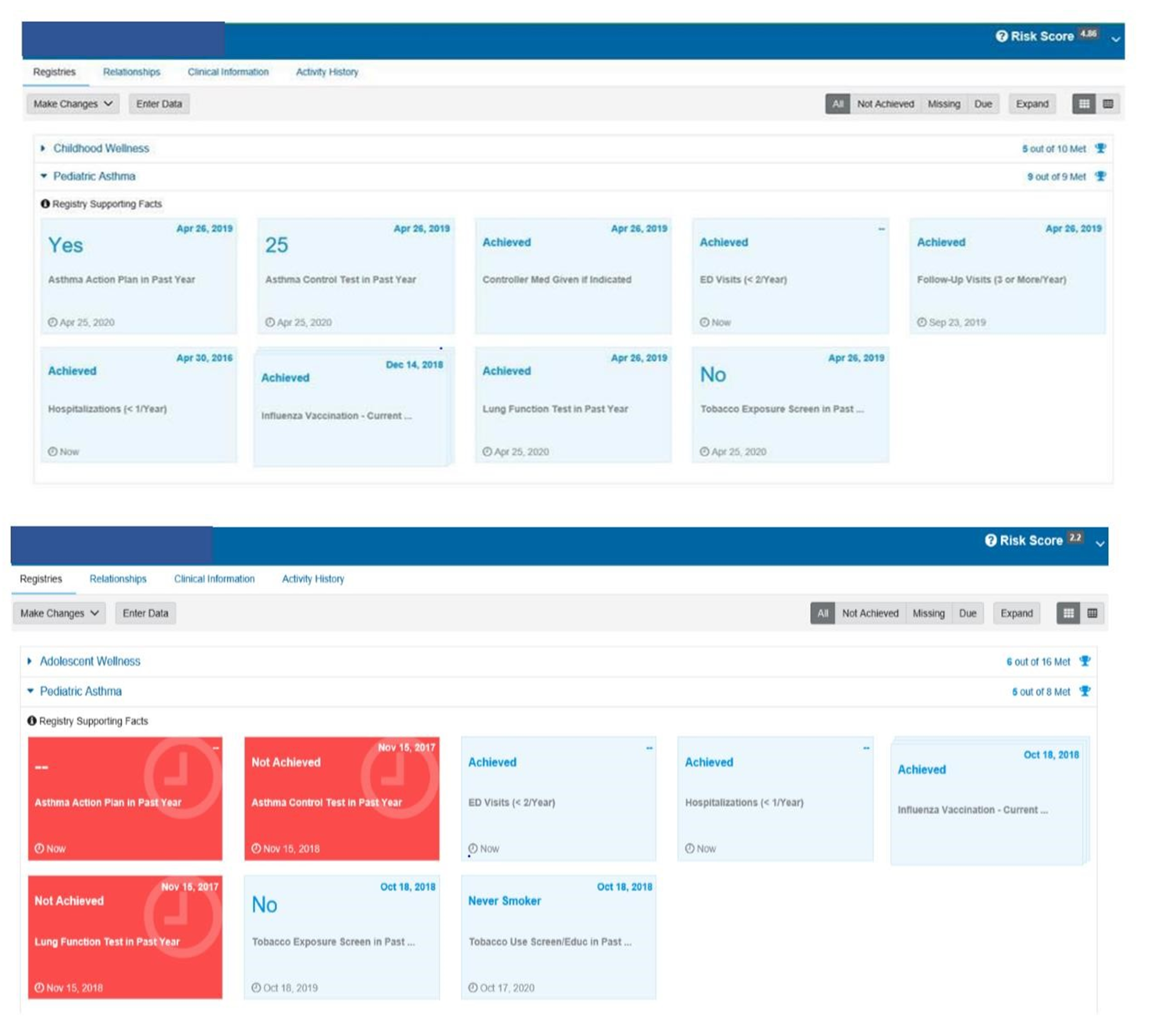
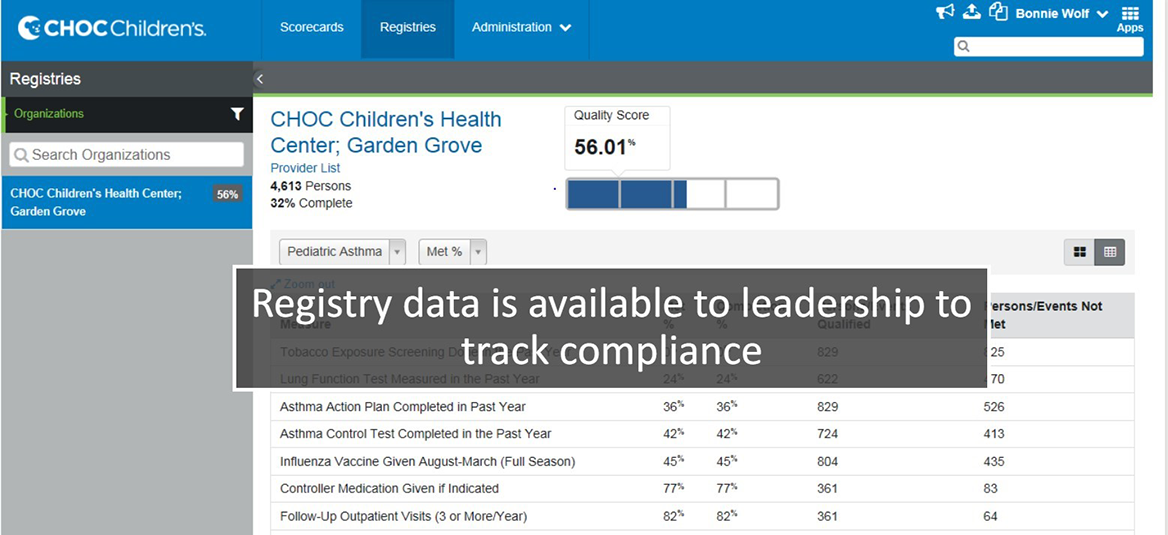
Based on the figures below, you can see a patient who has met all measures, compared to a patient who has some measures that have not been achieved.
Source: Children’s Hospital of Orange County
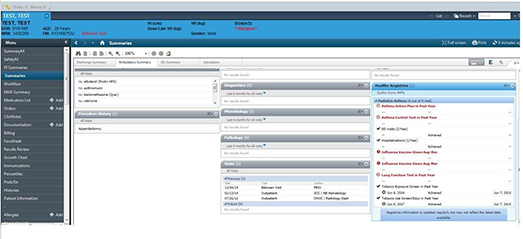
The provider’s view is a push of the registry requirements to the point of care within the workflow.
Source: Children’s Hospital of Orange County
The primary care team participated in a LEAN Kaizen event to gain an understanding of and improve upon the current state of asthma management. Care team education was based on a train-the-trainer format and materials included job aids, classroom time, online videos, tutorials, and elbow to elbow support during the rollout.
Following the importance of the design and implementation of the asthma registry, is access to care managers who are front and center receiving alerts, providing availability for telehealth visits, and working with the care team to keep everyone updated on their asthma population.
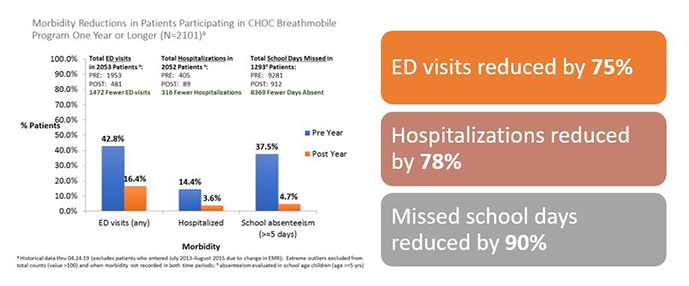
The organization is dedicated to keeping the pediatric asthma patient healthy, managing the disease holistically, and preventing exacerbations. CHOC is ranked as one of the top pulmonology programs in the nation by U.S. News & World Report. CHOC offers patient and family-centered care and comprehensive inpatient and outpatient management for children with asthma. The organization offers comprehensive asthma education by a certified asthma educator for families to learn how to manage and control asthma symptoms. CHOC proudly offer the Breathmobile, the only mobile asthma clinic serving preschool and school-aged kids in Orange County. CHOC also provides the only high-risk asthma clinic in the region dedicated to treating life-threatening asthma. The Breathmobile is another key to the success in reducing the ED visits and hospitalization. In 2019 alone, this team helped to reduce ED visits, hospitalizations, and missed school days.

Source: Children’s Hospital of Orange County
Source: Children’s Hospital of Orange County
Improving Adherence to the Standard of Care
A foundational component of CHOC Children’s Population Health program is the creation of a single patient-centered plan of care that can be used by the entire care team across the complete care continuum, including schools and the Breathmobile. The foundation of this care sits upon the population health platform which also supplies the data for the system review. The utilization of the population health platform empowers the team to take disparate sources of data (different electronic health records, claims, labs, pharmacy data, etc.) and transform the data in to meaningful, useful information and integrate the required documentation into the EHR. The results included (at top performance):
- In December 2019, ~59% of primary care patients received the asthma action plan—up from 28.89% in April 2017.
- In December 2019, 57% of primary care patients received the asthma control test—up from 29.61% in April 2017.
- Patients being seen in the ED for asthma deceased as well as the readmission rate within seven days of discharge per 100 patients decreased from 1.84 to 0.3. The numerators are respectively the patients who received the AAP and ACT, patients seen in the ED with the diagnosis of asthma. The denominator is the number of patients in the asthma registry with the diagnosis of asthma. The adherence to the standard of care in the use of the registry, the ACT, and the AAP, along with clinically driven evidenced-based processes which are managed by real-time analytics and standing meetings to address compliance has proven effective in driving outcomes and enhancing utilization of the tools.
Source: Children’s Hospital of Orange County
Improving Patient Outcomes
The organization implemented pediatric condition registries with an initial focus on pediatric asthma to be used by primary care providers. The organization increased and stabilized the number of primary care patients who received an AAP and ACT. This resulted in lower ED visits, seven-day readmissions, and overall readmissions for asthma. CHOC achieved these results by using analytical data on a monthly basis for transparency into how providers were performing against their value measures. The numerators are respectively the patients who received the AAP and ACT, patients seen in the ED with the diagnosis of asthma, and patients readmitted after seven days. The denominator is the number of patients in the asthma registry with the diagnosis of asthma.
Source: Children’s Hospital of Orange County
Source: Children’s Hospital of Orange County
Accountability and Driving Resilient Care Redesign
For a pediatric healthcare system, effective management of the pediatric asthma population improves the well-being of the patients and their families, reduces emergency department visits and improves overall health outcomes. With this goal in mind, physicians, IT leaders, and care management teams at Children’s Hospital of Orange County leveraged a population health registry to improve the health of pediatric asthma patients. As part of this registry, the CHOC Children’s team worked together to research and define measures that were appropriate for the care of pediatric asthma patients. Ten measures were defined and built into the population health asthma registry. Of these, two were selected for a focus on improvement—patients with an asthma control test completed in the past year and patients with an asthma action plan completed in the past year. Key factors for effectively using the measures and the patient registry was making the status of those measures available in real time in the clinical workflow and incorporating the registry data into the standard work of every patient encounter. For example, if a child who has asthma visits with a physician at a primary care clinic and that patient has not had an asthma control test in the past year, that information is front facing to the providers and the care teams. In addition, to track improvements, baseline data was documented, and dashboards were built to provide information on the completion of measures in real time. Since the care team can identify gaps in the service and respond proactively to close those gaps, the organization can maximize the ability to see patients more efficiently.
Along with the push of information directly to the point of care, CHOC also utilizes analytics to measure the compliance of registry and care guideline utilization. Each physician group and each physician are held accountable for care compliance. The organization can focus on local variations in care to reduce frequent ED visits and hospital admissions. CHOC is able to track improvements in compliance with registry metrics over time in reports, dashboards, and scorecards. A re-focus on the asthma registries in 2017 led to improved compliance and improved outcomes.
Source: Children’s Hospital of Orange County
The views and opinions expressed in this content or by commenters are those of the author and do not necessarily reflect the official policy or position of HIMSS or its affiliates.
HIMSS Davies Awards
The HIMSS Davies Award showcases the thoughtful application of health information and technology to substantially improve clinical care delivery, patient outcomes and population health.
Related

Patient Access
Articles

Davies Award of Excellence

Digital Health
Case Studies
